
This is why laser marking isn't a preference — it's the only marking method that satisfies both FDA regulatory requirements and the physical demands of surgical instrument environments.
This guide covers the regulatory framework driving laser marking requirements, the four marking techniques and when to use each, laser type selection by material, the passivation challenge that catches manufacturers off guard, and what process validation actually requires under ISO 13485.
Key Takeaways
- FDA's 21 CFR 801.45 requires a permanent UDI mark directly on reusable surgical instruments — packaging labels don't satisfy this requirement
- Laser annealing is the preferred technique for fluid-contact stainless steel and titanium surfaces because no material is removed
- The wrong laser recipe can reduce surface chromium by ~15% and trigger passivation failures; validate every process against your actual acid chemistry before production
- MOPA and picosecond fiber lasers offer better passivation resistance than standard fiber lasers for stainless steel
- ISO 13485 Clause 7.5.6 treats laser marking as a validated production process, so any parameter changes require formal revalidation
Why Laser Marking Is Required for Surgical Instruments
The Regulatory Foundation
The FDA's Unique Device Identification system is codified in 21 CFR Part 830, but the direct-marking obligation lives in 21 CFR 801.45(a). That section requires any reusable device — one that must bear a UDI label and is reprocessed between uses — to also carry a permanent UDI mark directly on the device itself.
Reusable instruments are routinely separated from their original packaging during use and reprocessing. Once that packaging is gone, the only remaining identifier is whatever is marked on the instrument itself.
UDI Structure: What the Mark Must Contain
A compliant UDI has two distinct components:
- Device Identifier (DI): The fixed portion — identifies the labeler and the specific device version or model. Every unit of the same model shares the same DI.
- Production Identifier (PI): The variable portion — includes lot/batch number, serial number, manufacturing date, expiration date, and where applicable, distinct identification codes for HCT/P devices.
Both components must appear in human-readable and machine-readable (AIDC) formats. For surgical instruments, this typically means a 2D Data Matrix code alongside a plain-text string — both permanently marked on the instrument surface.
Compliance Timeline by Device Class
| Device Class | Label + GUDID Submission | Direct Marking on Device |
|---|---|---|
| Class III | September 24, 2014 | September 24, 2016 |
| Class II | September 24, 2016 | September 24, 2018 |
These deadlines have passed. Manufacturers of reusable Class II and Class III instruments that haven't implemented direct marking are already out of compliance.
Why Other Methods Don't Work
- Adhesive labels: Fail during sterilization; cannot survive repeated autoclave cycles
- Inkjet/ink-based codes: Non-permanent, use chemicals not approved for patient-contact surfaces, and degrade with cleaning agents
- Mechanical pin-stamping: Creates raised or recessed surface features that trap bacteria and resist adequate cleaning
- Chemical etching: Cannot produce incremental serial numbers or 2D Data Matrix codes at production scale
The Traceability Advantage Beyond Compliance
A readable UDI on a defective instrument enables a targeted recall: manufacturers can trace the part to its production batch, identify the root cause, and notify only the affected facilities. Without device-level identification, the only option is a broad recall based on lot estimates — more disruptive, more costly, and harder to defend to regulators.
That's the practical value of permanent marking. It gives manufacturers the evidence chain needed to contain a problem rather than react to it.
Four Laser Marking Techniques for Surgical Instruments
| Technique | Material Removed? | Primary Medical Application | Biocompatibility Note |
|---|---|---|---|
| Annealing | No | Stainless steel, titanium surgical instruments | Preserves surface smoothness; validate passivation survival |
| Engraving | Yes (significant) | Orthopedic implants, abrasion-environment components | Deep recesses require bacterial entrapment evaluation |
| Etching | Minimal (surface melt) | Metal housings, hard polymer non-contact components | Not recommended for surfaces affecting tissue integration |
| Ablation | Yes (coating layer) | Anodized aluminum, coated cannulas, catheters | Validate per ISO 10993 for any patient-contact surface |
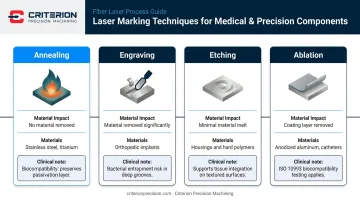
Laser Annealing
Annealing is the preferred method for stainless steel and titanium surgical instruments. The laser applies controlled heat to produce a dark subsurface oxide layer: no material is removed, the surface stays smooth, and no crevices form that could harbor bacteria. As TRUMPF describes it, the result is an oxide film with no surface disruption — making this the default choice for fluid-contact and implant-grade surfaces under ISO 13485.
Critical caveat: Not every annealing recipe preserves the chromium oxide passivation layer. The marking process must be validated against your specific passivation method. More on this below.
Laser Engraving
Engraving removes material to create physically recessed marks, durable and readable even after aggressive surface treatments like shotblasting. It's appropriate for orthopedic implants or components that don't contact body fluids directly.
Depth specification is engineering-driven, determined by three factors:
- Readability after sterilization cycles
- Cleaning validation — deeper recesses require bacterial entrapment evaluation
- Fatigue risk — depth affects stress concentration in load-bearing components
There is no universal regulatory threshold; the specification is application-specific.
Laser Etching
A faster, high-contrast option that creates shallow surface texture through minimal material melt. Suited for metal housings and hard polymer components that don't contact body fluids or undergo abrasive sterilization. For any patient-contact surface, topographic effects on tissue integration must be evaluated before specifying etching.
Laser Ablation
Ablation removes a coating or surface layer to reveal a contrasting substrate beneath. Common applications include anodized aluminum components, coated cannulas, and catheters — including depth-banding marks that indicate insertion depth during a procedure. Any ablated surface that contacts the patient requires biological evaluation per ISO 10993 before the marking process is locked into the device record.
Choosing the Right Laser Type by Material
Standard Fiber Laser (1,064 nm)
Pulsed 1,064 nm fiber lasers are strongly absorbed by metals and serve as the baseline for marking stainless steel, titanium, and aluminum. They deliver fast marking on common surgical alloys.
Parameter optimization matters on corrosion-critical stainless steel. Applied incorrectly, standard fiber lasers can create chromium-depleted zones at mark boundaries that initiate corrosion during passivation.
MOPA and Picosecond Fiber Lasers
For stainless steel UDI compliance, pulse-duration control matters. MOPA (Master Oscillator Power Amplifier) lasers add this control, enabling true annealing through precise thermal management. Picosecond lasers go further: ultrashort pulses create high-contrast black marks that Amada Weld Tech's testing shows are resistant to passivation, corrosion, and autoclaving.
Across published sources, minimizing and controlling heat input is what produces marks that survive passivation. Whether you use MOPA, picosecond, or UV nanosecond matters less than validating that your chosen process passes your actual passivation chemistry.
UV Laser (355 nm)
UV lasers at 355 nm mark medical plastics through photochemical reaction rather than thermal ablation — often called "cold marking." Surface temperatures stay low enough to mark PEEK implants, polycarbonate tubing connectors, medical-grade silicone, and cannulas without thermal damage to heat-sensitive structures. For Class II polymer components where a fiber laser's heat would compromise the material, UV is the right tool.
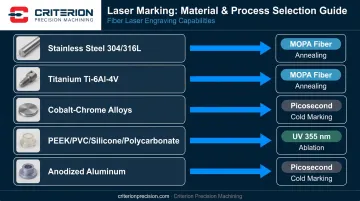
Material-to-Laser Reference
| Material | Recommended Laser Type | Process |
|---|---|---|
| Stainless steel 304/316L | MOPA fiber or picosecond | Annealing |
| Titanium alloys (Ti-6Al-4V) | MOPA fiber | Annealing |
| Cobalt-chrome alloys | Fiber or MOPA | Annealing/etching, validate per alloy |
| PEEK, PVC, polycarbonate, silicone | UV (355 nm) | Cold marking/ablation |
| Anodized aluminum | Fiber or UV | Ablation |
Laser Marking and Passivation: What Manufacturers Must Know
Why Passivation Matters — and Where It Goes Wrong
After machining stainless steel, iron particles embedded in the surface during cutting degrade the protective chromium oxide layer. Passivation — using citric or nitric acid per ASTM A967 — removes those iron particles and rebuilds the passive layer. This is standard practice for surgical instrument manufacturing.
The problem: laser heat can locally reduce chromium concentration at the mark boundary. When passivation acid contacts that chromium-depleted zone, it etches the mark away rather than treating the surrounding steel. You pass dimensional inspection, apply your UDI mark, run passivation — and the mark is gone or illegible. Amada Miyachi's EDX analysis found that failed marks showed approximately 15% lower chromium concentration than surrounding unaffected material. That deficit is what the passivation acid attacks.
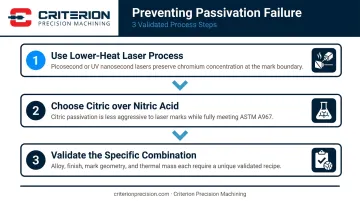
How to Solve It
Three approaches reduce this risk:
- Use a lower-heat laser process — Picosecond or UV nanosecond lasers deposit less heat more uniformly, preserving sufficient chromium to survive passivation
- Use citric acid over nitric acid — Citric acid is less aggressive to laser marks while still meeting ASTM A967 requirements; nitric acid is more likely to degrade borderline marks
- Validate the specific combination — There is no universal parameter set. Each instrument alloy, surface finish, mark geometry, and thermal mass combination requires its own validated recipe
No Universal Parameters Exist
Astropak's analysis of laser-marked medical stainless is unambiguous: the laser mark, stainless alloy, and passivation process interact, and manufacturers must develop and validate the actual marking-plus-passivation sequence for their specific instruments. Starting parameters from a laser supplier give you a baseline. A qualified process requires documented validation against your alloy, finish, and passivation chemistry.
Process Validation and Quality Standards
ISO 13485 Clause 7.5.6
Under ISO 13485, laser marking is a production process that affects product quality and must be validated. Clause 7.5.6 (Validation of processes for production and service provision) requires documented evidence that a specific laser setup, on a specific instrument material and surface finish, produces marks meeting defined acceptance criteria — including legibility after all sterilization cycles, passivation exposure, and handling conditions specified for that instrument.
This means validation must demonstrate:
- Mark legibility after the maximum specified number of sterilization cycles
- Mark survival through the complete passivation process
- No degradation of surface biocompatibility per ISO 10993
- Consistent AIDC readability meeting the scanner grade requirements in the UDI specification
Revalidation Requirements
Any change to a validated marking process — laser equipment model, software version, optics, parameter adjustments, passivation chemistry, or material lot — requires a formal change control assessment and, typically, revalidation. The IMDRF/GHTF process validation guidance addresses exactly this: changes that can affect validated outputs require review and documented revalidation determination.
In practice, this means marking equipment changes aren't just procurement decisions. They're quality events requiring IQ/OQ/PQ protocols.
What ISO 13485 Certification Signals
An ISO 13485-certified machining supplier already operates within a compliant quality management framework: documented process controls, change control procedures, production records, and validation requirements built into daily operations. For medical device OEMs selecting a precision machining partner who also handles or specifies the marking step, that certification is meaningful evidence that the supplier understands process discipline — not just dimensional accuracy.
Criterion Precision Machining holds ISO 13485:2016 certification and machines titanium, stainless steel, and cobalt-chrome alloys for medical device customers including Riverpoint Medical and Smith & Nephew. Key capabilities relevant to validation include:
- In-house fiber laser marking on a FOBA M3000 system, keeping the marking step within the same quality management system as machining
- Production-intent prototyping that runs prototypes on the same equipment and inspection systems used for full production, reducing revalidation burden during scale-up
- Integrated change control procedures covering both machining and marking processes within a single ISO 13485:2016 QMS

What to Look for in a Precision Machining Partner
Laser marking decisions cannot be separated from machining decisions. Surface finish, alloy grade, part geometry, and post-machining treatments all directly affect which marking process and parameters will produce a compliant, durable mark. A supplier who understands these interdependencies catches problems before validation testing begins, not after a failed qualification run.
Key qualifications to evaluate:
- ISO 13485 certification confirms a quality management system built specifically for medical device production, not adapted from general manufacturing
- Alloy-specific experience — stainless 316L, titanium alloys, and cobalt-chrome each behave differently under laser and passivation conditions; ask for documented evidence with your specific material
- In-house laser marking reduces process-parameter drift between machining and marking, and keeps traceability records under a single quality system
- Passivation coordination matters whether it's in-house or subcontracted; the supplier should show marking parameters validated against the actual acid chemistry used
- FDA documentation familiarity — look for working knowledge of 21 CFR Part 830, 21 CFR 801.45, DI/PI data structure, and device history record requirements
- Formally validated IQ/OQ/PQ records, not just "we've done it before" — ask to see the documentation
The right partner brings all of these capabilities under one roof. That integration — machining, marking, passivation, and documentation — is what keeps a UDI program on schedule and out of corrective action.
Frequently Asked Questions
What is laser marking for surgical instruments?
Laser marking uses a focused beam to permanently mark surgical instruments with identification codes, serial numbers, and 2D Data Matrix codes without inks, adhesives, or mechanical stamping. The resulting marks are biocompatible, sterilization-resistant, and machine-readable — satisfying FDA UDI requirements under 21 CFR 801.45 and process control requirements under ISO 13485.
What laser type is best for marking stainless steel surgical instruments?
MOPA fiber lasers and picosecond lasers are the preferred choices because their pulse-duration control enables true annealing — a subsurface color change with no material removal — that preserves the chromium oxide passivation layer. Standard fiber lasers applied without precise parameter control can create chromium-depleted zones that fail passivation testing.
How does laser marking affect passivation of stainless steel instruments?
Laser heat can locally reduce chromium concentration at the mark boundary — when passivation acid contacts this depleted zone, it etches the mark rather than treating the steel. The fix is a lower-heat process (MOPA, picosecond, or UV nanosecond) with validated parameters for each instrument alloy and acid chemistry.
What is the difference between laser annealing and laser engraving for surgical instruments?
Laser annealing creates a dark subsurface color change with no material removal — preserving surface smoothness and the passive layer. Laser engraving removes material to create a recessed mark. Annealing is preferred for fluid-contact and implant-grade surfaces; engraving is appropriate for instruments in abrasive environments where surface smoothness isn't a biocompatibility concern.
Which surgical instruments must carry a UDI mark?
Under 21 CFR 801.45, reusable devices that bear a UDI label and are reprocessed before each use must carry a permanent direct mark on the device itself. Class III instruments have required direct marking since 2016; Class II instruments since 2018.
Does laser marking affect the biocompatibility of surgical instruments?
Laser annealing, when correctly applied, creates a stable oxide layer, leaves no residue, and introduces no foreign materials — maintaining biocompatibility. However, manufacturers must validate that their specific marking process doesn't alter surface chemistry in ways that affect biological safety, per ISO 10993 biological evaluation requirements for patient-contact surfaces.


