
The wide variety of fastener types, materials, and thread geometries isn't arbitrary. Each design solves a specific mechanical problem: gripping dense cortical bone versus soft trabecular bone, enabling fluoroscopic-guided placement, or avoiding hardware prominence on an articular surface. Choosing the wrong fastener for the fracture pattern or anatomical location compromises fixation and delays healing.
This article covers the major orthopedic fastener types, the materials they're made from, their clinical applications, and the manufacturing precision required to make them safe and effective.
Key Takeaways
- Orthopedic fasteners convert mechanical loads into stable fixation — the foundation of bone healing
- Cortical, cancellous, locking, cannulated, lag, and headless screws each solve a distinct mechanical problem
- Material choice determines imaging compatibility, long-term biocompatibility, and whether hardware removal surgery will be required
- Thread geometry, core diameter, and surface finish directly determine pullout strength and torsional yield
- ISO 13485 certification and ±0.0002" tolerances are non-negotiable minimums for Class II implantable orthopedic components
What Are Orthopedic Fasteners?
Orthopedic fasteners are the class of implantable hardware — screws, bone plates, washers, and associated bolt nuts — used in internal fixation to hold fractured or reconstructed bone in proper alignment during healing.
A fastener converts rotational driving torque into axial compression across a fracture or joint surface. That compression creates the stability bone cells need to regenerate.
Without adequate fixation, micromotion at the fracture site prevents union and increases infection risk.
Regulatory Classification
Under U.S. FDA regulation, orthopedic fasteners fall into distinct Class II categories:
- Bone screws — product code HWC, 21 CFR 888.3040, "Smooth or threaded metallic bone fixation fastener"
- Bone plates — product code HRS, 21 CFR 888.3030, "Single/multiple component metallic bone fixation appliances and accessories"
- Washers and bolt nuts — product codes HTN and NDG, 21 CFR 888.3030
All require FDA 510(k) premarket notification. The FDA's 2024 final guidance on non-spinal bone plates, screws, and washers defines what's required for 510(k) submissions. That includes dimensional accuracy, material traceability, and manufacturing quality documentation.
Types of Orthopedic Fasteners
Orthopedic fasteners span three primary hardware families — bone screws, bone plates, and washers — each containing distinct sub-types suited to different mechanical roles. Bone density, anatomical location, fracture geometry, and fixation strategy all drive the hardware selection.
Bone Screws: Cortical, Cancellous, and Lag Types
Three screw types dominate cortical and cancellous fixation, each defined by thread geometry:
- Cortical screws — fine-pitch, closely spaced, shallow threads engineered for the dense outer shell (cortex) of long bones
- Cancellous screws — deep, widely spaced threads that grip softer trabecular bone in metaphyseal and epiphyseal zones
- Lag screws — achieved with a partially threaded cancellous screw or a fully threaded cortical screw with an over-drilled near cortex, creating interfragmentary compression by gripping only the far fragment while the near fragment slides freely
The core distinction is thread geometry matched to bone density:
| Screw Type | Thread Geometry | Primary Application | Common Diameters |
|---|---|---|---|
| Cortical | Fine pitch, fully threaded | Diaphyseal plating (humerus, forearm, tibia) | 2.7mm, 3.5mm, 4.5mm |
| Cancellous | Deep, wide thread, often partially threaded | Metaphyseal/periarticular fixation, femoral neck | 6.5mm (4.0mm core) |
| Lag | Either type, over-drilled near cortex | Interfragmentary compression, epiphyseal fractures | Varies by location |
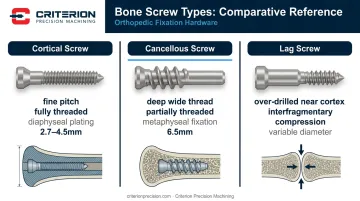
Key limitations: Cortical screws placed in soft cancellous bone will strip and lose purchase. Cancellous screws in very dense cortex may not engage enough thread turns to resist pullout under load.
Locking, Cannulated, and Headless Compression Screws
Locking screws have threaded heads that engage matching threads in the plate hole, making the screw-plate interface a fixed-angle construct (an internal fixator) rather than relying on friction between plate and bone.
Cannulated screws carry a hollow core for placement over a guidewire under fluoroscopic imaging, enabling precise trajectory control in anatomically difficult locations. Headless compression screws use differential thread pitch (coarser at the leading end, finer at the trailing end), so the implant buries entirely beneath the bone surface.
Best-suited applications:
- Locking screws — osteoporotic bone, periarticular fractures, minimally invasive plate osteosynthesis (MIPO). The fixed-angle construct distributes load across the entire plate-screw system, not the bone surface.
- Cannulated screws — femoral neck fractures, scaphoid fractures, any location where fluoroscopic guidewire positioning is critical.
- Headless compression screws — intra-articular fractures (scaphoid, capitellum, osteochondral fragments) where hardware prominence would damage opposing cartilage.
Locking plates cost more than conventional compression plates. Using locking screws where conventional fixation would suffice adds expense without clinical benefit. Cannulation slightly reduces core diameter, marginally affecting fatigue resistance.
Bone Plates and Washers
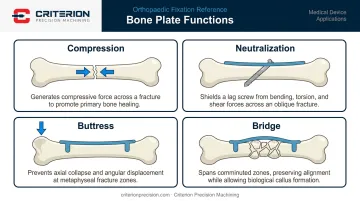
Screws anchor force to bone, but the plate governs the mechanical environment of the healing fracture. Depending on how a plate is applied, it serves one of four distinct functions:
- Compression — DCP plate holes use inclined geometry to translate the bone fragment as the screw tightens, compressing the fracture
- Neutralization — protecting a lag screw construct from bending and rotational forces
- Buttress — resisting axial collapse of a depressed fragment (tibial plateau fractures)
- Bridge — spanning comminuted zones while maintaining alignment, promoting callus formation
Washers distribute load from the screw head across a broader bone surface area, reducing the risk of screw-head subsidence into soft bone. An AO-documented example: washers paired with lag screws prevent screw advancement through thin lateral tibial head cortex.
Together, plates and screws form a unified construct: the plate sets the load-sharing geometry; the screws transfer that load to bone.
Materials Used in Orthopedic Fasteners
Material selection determines biocompatibility, imaging compatibility, mechanical performance, and whether the device needs surgical removal.
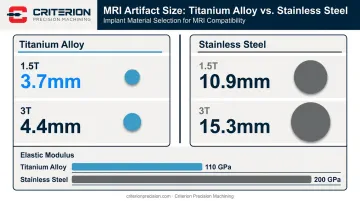
Titanium Alloys
Ti-6Al-4V (ASTM F136) and Ti-6Al-7Nb (ASTM F1295) dominate modern orthopedic fasteners. Key properties:
- Elastic modulus ~110 GPa — closer to cortical bone (7–30 GPa) than stainless steel, reducing stress shielding
- Superior biocompatibility with minimal ion release
- Substantially smaller MRI artifacts: peer-reviewed imaging data shows titanium alloy screws produce artifacts of 3.7mm at 1.5T and 4.4mm at 3T, versus 10.9mm and 15.3mm for stainless steel
Titanium is harder to machine than stainless steel, requiring controlled tooling, feeds, and coolant strategies to hold thread tolerances without work-hardening the surface. Criterion Precision Machining's Swiss turning centers — configured in 5-, 6-, and 8-axis arrangements with live tooling — machine titanium orthopedic screws to ±0.0002" tolerances. That dimensional consistency is what thread features require to deliver predictable pullout strength.
Stainless Steel
Where titanium prioritizes imaging performance and stress distribution, 316L stainless steel (ASTM F138, UNS S31673) trades those advantages for lower cost and easier machinability. It remains in active use for instruments, reconstruction plates, and cost-sensitive applications.
Key characteristics:
- Elastic modulus ~200 GPa — stiffer than titanium, which increases stress shielding risk with long-term implantation
- Easier and less expensive to machine than titanium alloys
- Handles intraoperative contouring without fracture
Critical rule: Never mix titanium and stainless steel in the same construct. The dissimilar metals create galvanic corrosion in the biological environment, releasing metallic ions and accelerating implant degradation.
PEEK and CFR-PEEK
PEEK (ASTM F2026) and carbon fiber-reinforced PEEK (CFR-PEEK, ASTM F3333) offer an elastic modulus of 3.7–4.0 GPa — closer to cortical bone than either metal. PEEK is radiolucent, enabling clearer post-operative imaging and no galvanic reaction risk. CFR-PEEK adds directional stiffness through fiber reinforcement.
Manufacturing note: fiber direction and fiber percentage in CFR-PEEK directly affect mechanical performance and must be controlled and documented throughout production.
Bioabsorbable Polymers
Polylactic acid (PLA), polyglycolic acid (PGA), and their copolymers (PLGA) are used where avoiding a second removal surgery is the priority — pediatric fixation near growth plates, soft-tissue-to-bone fixation, and osteochondral repair.
Degradation timelines differ by polymer:
- PGA — complete degradation in 6–12 months; loses mechanical strength rapidly
- PLLA — degrades over several years; used in load-bearing applications
- PLGA (85L:15G) — mostly absorbed in 12–16 months, largely dissolved by 2 years
The critical trade-off: bioabsorbable screws have lower initial mechanical strength than metallic screws. Premature degradation before union causes fixation failure; very slow degradation prolongs foreign body reaction.
Clinical Applications of Orthopedic Fasteners
The global trauma devices market reached USD $14.87 billion in 2024, projected to grow to $23.59 billion by 2033 at a 5.30% CAGR — a market driven primarily by orthopedic fracture fixation volume.
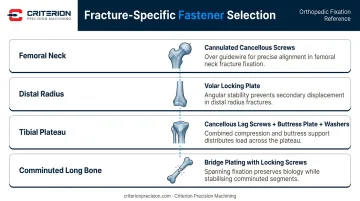
Fracture Fixation
Fastener choice is fracture-specific:
- Femoral neck fractures — cannulated 6.5mm or 7.0–7.3mm cancellous screws placed over fluoroscopic guidewires
- Distal radius fractures — volar locking plates with angular stable fixation, particularly useful in osteoporotic bone
- Tibial plateau fractures — cancellous lag screws for subchondral support, buttress plate for split components, washers where cortex is thin
- Comminuted long-bone fractures — bridge plating with locking screws spanning the comminuted zone
Joint Reconstruction and Arthrodesis
Each application in this category carries distinct fastener geometry demands:
- Wrist, foot, and ankle arthrodesis — lag screws and headless compression screws for joint compression and fusion
- Spinal fixation — pedicle screws requiring precise thread engagement in cancellous vertebral bone
- Total hip arthroplasty — acetabular cup fixation screws managing both primary stability and long-term osseointegration
Sports Medicine and Soft-Tissue Repair
Suture anchors — classified as fasteners under FDA regulatory guidelines — for labral repair, rotator cuff repair, and ACL reconstruction are predominantly PEEK, biocomposite, or titanium. Sizes range from 2.9mm to 5.5mm depending on anatomical location, per FDA 510(k) clearances for suture anchor systems.
This segment is pushing precision requirements smaller. Implants at 1.3–2.5mm diameter demand Swiss turning capabilities and rigorous inspection. For contract machining suppliers, this is a critical capability threshold — Criterion's Swiss turning range spans 0.04" to 0.875" (approximately 1.0mm to 22.2mm), covering these specifications fully.
Selecting the Right Orthopedic Fastener
Fastener selection is governed by four intersecting factors:
- Bone quality — density and vascularity at the fixation site
- Fracture pattern — simple vs. comminuted, transverse vs. oblique
- Anatomical location — cortical diaphysis vs. cancellous metaphysis vs. intra-articular surface
- Patient factors — age, activity level, osteoporosis, weight-bearing compliance
Common Selection Errors
Avoid these mistakes:
- Using cortical screws in cancellous bone zones (thread stripping, loss of purchase)
- Choosing locking constructs for simple diaphyseal fractures in healthy bone where conventional compression is more appropriate and less expensive
- Selecting material based on cost rather than the clinical environment (MRI follow-up anticipated? Use titanium.)
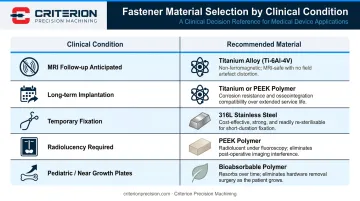
Material Selection Logic
| Clinical Condition | Recommended Material |
|---|---|
| MRI follow-up anticipated | Titanium alloy |
| Long-term implantation planned | Titanium alloy |
| Temporary fixation, healthy patient | 316L stainless steel |
| Radiolucency or imaging clarity required | PEEK |
| Pediatric patient near growth plates | Bioabsorbable polymer |
Manufacturing Quality: The Non-Negotiable Variable
A fastener's design performance is only as reliable as the precision with which it was manufactured. Dimensional non-conformance in thread pitch, core diameter, or surface finish directly affects pullout strength, torsional yield, and biocompatibility. Orthopedic screws are Class II medical devices — the supply chain must reflect that.
Criterion Precision Machining holds ISO 13485:2016 and ISO 9001 certifications and manufactures orthopedic components in titanium, stainless steel, and PEEK to tolerances as tight as ±0.0002". Capabilities include:
- Screws via Swiss turning
- Plates via 5-axis milling
- Production-intent prototyping on the same machines and tooling used in full production runs
- Complete traceability through ProShop ERP: incoming material verification, first article inspection, in-process checks, and final inspection before shipment
Frequently Asked Questions
What kind of screws do orthopedic surgeons use?
Orthopedic surgeons use cortical, cancellous, locking, and cannulated screws, selected based on fracture location, bone density, and the mechanical goal. Cortical screws grip dense diaphyseal bone; cancellous screws anchor in softer metaphyseal zones; locking screws create fixed-angle constructs independent of bone contact; cannulated screws enable guidewire-assisted placement under fluoroscopy.
How long do screws stay in after surgery?
Metallic screws are often left permanently in place if they cause no symptoms. When removal is indicated, most implants are extracted within 24 months of surgery. Bioabsorbable screws dissolve over months to years depending on polymer composition, eliminating the need for a second operation entirely.
What is the difference between locking and conventional bone screws?
Conventional screws rely on friction between the plate and bone surface for stability, requiring direct periosteal contact. Locking screws thread directly into the plate, creating a fixed-angle construct independent of bone contact, making them the standard choice for osteoporotic bone and periarticular fractures where friction-based purchase is unreliable.
What materials are most commonly used in orthopedic fasteners?
The four main materials are:
- Ti-6Al-4V (ASTM F136) — most modern implants
- 316L stainless steel (ASTM F138) — instruments and cost-sensitive applications
- PEEK (ASTM F2026) — where radiolucency and imaging clarity matter
- Bioabsorbable polymers (PLA, PGA, PLGA) — where avoiding removal surgery is the priority
Can titanium and stainless steel implants be mixed in the same construct?
No. Mixing titanium and stainless steel in one construct creates galvanic corrosion in the biological environment. The electrochemical reaction releases metallic ions, accelerates implant degradation, and causes tissue reaction and pain. All hardware within a single fixation construct must be the same material.
What manufacturing tolerances are required for orthopedic implant screws?
Orthopedic screws require tightly controlled thread pitch, core diameter, major and minor diameter, and surface finish — machining tolerances of ±0.0002" are common. ASTM F543 governs torsional yield strength, maximum torque, and breaking angle; ISO 13485 certification is required for FDA 510(k) submissions.


