Introduction
Titanium has become so dominant in dental implant manufacturing that it's difficult to imagine an alternative. According to Grand View Research, titanium accounted for 91.0% of dental implant revenue share in 2025, within a global market valued at $7.82 billion. That concentration reflects decades of clinical validation, material science, and precision manufacturing arriving at the same conclusion.
What follows is a practical look at the material properties, clinical applications, and manufacturing requirements behind titanium implants — and why getting the machining right is as important as the biology.
Key Takeaways
- Titanium holds 91% of the dental implant market due to proven osseointegration, biocompatibility, and corrosion resistance
- Grade 5 Ti-6Al-4V ELI delivers 860 MPa tensile strength — roughly 56% stronger than Grade 4 CP titanium — making it the dominant alloy for load-bearing implants
- SLA surface-treated implants report 96.1% cumulative survival at 12 years
- Long-term systematic reviews show 93% implant survival after 20+ years
- Producing implants to these clinical standards demands machining tolerances as tight as ±.0002" and ISO 13485-compliant quality systems throughout production
What Are Titanium Dental Implants?
Structure and Function
A dental implant is a three-part system:
- The fixture — a titanium post surgically inserted into the jawbone, functioning as an artificial tooth root
- The abutment — a connector piece that attaches to the top of the fixture and supports the prosthetic tooth
- The crown — the visible prosthetic tooth, typically ceramic or porcelain
Titanium is used primarily for the fixture and often the abutment. The crown is almost always ceramic.
What separates implants from bridges and dentures is that they're anchored inside the jawbone. That direct bone contact stimulates the jaw, helping preserve bone volume over time. Research comparing implant-supported prostheses to conventional dentures found that conventional dentures showed measurably higher vertical maxillary bone resorption — a clinically significant difference for long-term jaw health.
The Origin: Osseointegration
The modern implant traces back to Swedish orthopedic surgeon Per-Ingvar Brånemark, who discovered in 1952 that living bone could fuse directly to titanium, a phenomenon he named osseointegration. In 1965, he placed the first successful titanium dental implant in a human patient. That discovery established the biological foundation for implant protocols still used today.
Osseointegration means bone grows onto the implant surface without an intermediate fibrous tissue layer. The result is a mechanically stable, biologically integrated anchor that behaves more like a natural tooth root than any alternative.
What Are Titanium Dental Implants Made Of?
Early implants used commercially pure (CP) titanium, which offered excellent biocompatibility but proved too soft for sustained chewing forces. That limitation pushed the field toward titanium alloys, which deliver superior mechanical performance while preserving the biocompatibility that makes titanium viable as an implant material.
Grades of Titanium Used in Dental Implants
Two grades dominate dental implant manufacturing:
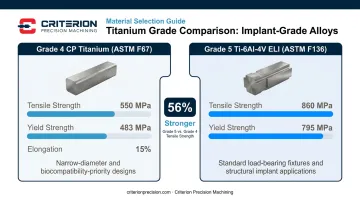
Grade 4 CP Titanium (ASTM F67)
- Highest-purity grade still used in implants
- Tensile strength: 550 MPa | Yield strength: 483 MPa | Elongation: 15%
- Favored in narrow-diameter designs where maximum biocompatibility matters more than peak mechanical load capacity
Grade 5 Ti-6Al-4V ELI (ASTM F136)
- Contains 6% aluminum and 4% vanadium
- Tensile strength: 860 MPa | Yield strength: 795 MPa
- The ELI (Extra Low Interstitial) variant reduces oxygen and iron content, further improving fatigue resistance and biocompatibility
- The standard choice for most load-bearing implant fixtures
Grade 5 delivers roughly 56% higher tensile strength than Grade 4, a difference that directly affects long-term performance in load-bearing applications.
Surface Treatments and Coatings
Material selection determines structural performance, but surface texture governs osseointegration — how effectively bone bonds to the implant. Surface modification is applied after machining:
- SLA (Sandblasted, Large-grit, Acid-Etched) — Large-grit blasting followed by acid etching creates a roughened micro-topography that accelerates early bone anchorage. A 12-year clinical study of SLA dental implants reported 96.1% cumulative survival and 1.18 mm mean marginal bone loss — strong long-term data.
- Hydroxyapatite (HA) coatings — HA-coated surfaces promote protein absorption, osteoblast adhesion, and bone growth, making them effective for applications where faster biological integration is a priority
- Anodization — Electrochemical process that thickens and modifies the oxide layer, influencing surface chemistry and roughness
Key Properties That Make Titanium the Gold Standard
Osseointegration
Osseointegration is titanium's defining clinical property. Bone grows directly onto the implant surface — no fibrous capsule, no rejection layer. Long-term systematic review data shows a 93.0% implant survival rate after 20+ years (95% CI: 91.6–94.1%). That's a multi-decade performance record backed by clinical evidence.
Biocompatibility
When titanium is exposed to oxygen, it forms a stable titanium dioxide (TiO₂) oxide layer almost instantly. This passive layer is chemically inert, preventing metal ions from releasing into surrounding tissue. Because the body does not recognize titanium as foreign, it does not mount a rejection response.
Corrosion Resistance
The same TiO₂ layer that ensures biocompatibility also protects against the oral environment's corrosive conditions — saliva, pH fluctuations, enzymatic activity. Stainless steel, by contrast, can suffer localized corrosion in physiological environments. Titanium alloys are specifically selected for their resistance to these conditions, which directly contributes to implant longevity.
Mechanical Advantages
Longevity under chemical attack is one thing; holding up under daily mechanical load is another. Titanium's mechanical profile is well-matched to both demands:
- High strength-to-weight ratio
- Fatigue resistance under cyclic chewing loads (thousands of load cycles daily)
- Elastic modulus closer to cortical bone than most metals, reducing stress-shielding effects
Ti-6Al-4V has an elastic modulus of roughly 110 GPa, compared with human cortical bone at 10–40 GPa. The gap exists, but it's meaningfully narrower than alternatives like cobalt-chrome alloys.
MRI Compatibility
Titanium is paramagnetic, not ferromagnetic. It does not interact with MRI magnetic fields in any clinically significant way, does not produce meaningful imaging artifacts, and carries no established safety risk during MRI scanning. Most titanium implants are considered MRI-compatible — though patients should confirm specific device labeling with their clinician, since individual product configurations vary.
Clinical Applications of Titanium Dental Implants
Titanium implants support a range of clinical scenarios — from replacing a single missing tooth to rehabilitating an entirely edentulous arch. Each application leverages the material's osseointegration properties differently, with prosthetic design and fixture placement adapted to available bone and patient anatomy.
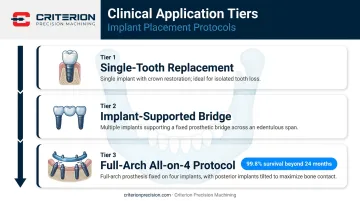
Single-Tooth Replacement
The most common application. A single titanium fixture supports one crown. Two-piece designs — where the abutment is separate from the fixture — allow angular placement adjustments to maximize use of available bone, an advantage in patients with non-ideal ridge anatomy.
Implant-Supported Bridges and Full-Arch Restorations
Multiple titanium implants anchor fixed bridges replacing several consecutive teeth. Full-arch concepts extend this further: the All-on-4 protocol uses four strategically placed implants — with the two posterior fixtures typically tilted up to 45 degrees — to support a complete prosthetic arch. Systematic reviews report 99.8% implant survival beyond 24 months for All-on-4 configurations, making this one of the better-documented full-arch approaches available.
Specialty Applications
| Application | Clinical Indication | Notes |
|---|---|---|
| Implant-supported overdentures | Patients needing removable full dentures stabilized by implants | Mini implant (MDI) studies show 93% survival at 10 years |
| Zygomatic implants | Severe maxillary atrophy where conventional implants lack bone | 96.2% mean survival at 6 years; sinusitis reported in ~14% at 5 years |
| Mini-implants | Narrow ridges or insufficient bone width | Typically Grade 5 Ti-6Al-4V; diameter as small as 1.8–2.4 mm |
Precision Manufacturing of Titanium Dental Implants
Why Titanium Is Difficult to Machine
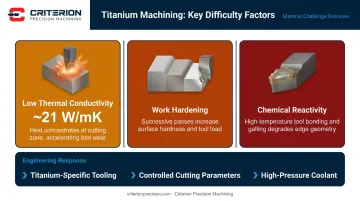
Titanium's material advantages in the body become challenges on the shop floor. Three properties make it notoriously demanding:
- Low thermal conductivity (~21 W/mK) — heat concentrates at the cutting zone rather than dissipating through the workpiece or chip
- Work hardening — the material hardens during cutting, increasing tool wear with each pass
- Chemical reactivity — at high cutting temperatures, titanium bonds to tool materials, causing galling, welding, and smearing
These characteristics demand titanium-specific tooling, controlled cutting parameters, high-pressure coolant, and manufacturing teams that understand how the material behaves under cutting conditions, not just what its datasheet says.
CNC Processes for Implant Components
Dental implant fixtures and abutments are machined using two primary processes:
CNC Turning creates the cylindrical implant body, thread profile, and overall fixture geometry. Thread pitch, lead angle, and minor diameter directly affect how bone contacts and integrates with the implant — so dimensional accuracy here carries direct clinical consequences.
Multi-Axis CNC Milling (4- and 5-axis) handles complex abutment geometries, internal connection features, and components requiring machined detail on multiple faces. Five-axis capability is now standard for modern abutment designs.
For the narrowest diameter implant components — mini-implants, narrow-body fixtures — Swiss turning delivers the precision these parts require. Swiss-style CNC machines hold extremely tight tolerances on slender, small-diameter parts, which is why they're a core capability for implant contract manufacturers. Criterion Precision Machining's Swiss turning centers, for example, machine diameters as small as .010" while holding tolerances to ±.0002".
Tolerance Requirements
Dental implant components require tolerances measured in thousandths of an inch. The implant-to-abutment connection is the most demanding interface: in vitro testing has measured implant-abutment microgaps of 0.3–9 μm before loading in precision-fit internal connections. Gaps at this scale harbor bacteria and contribute to peri-implant disease — which is why dimensional accuracy is a patient safety issue, not a line item on an inspection report.
Criterion Precision Machining holds tolerances as tight as ±.0002" for medical components, supported by a Global Advantage CMM with PC-DMIS software, a Keyence IM-series Image Dimension Measurement System, and an OASIS optical inspection system.
Quality Systems and Regulatory Requirements
Dental implant fixtures are FDA Class II devices (21 CFR 872.3640, product code DZE). Abutments are also Class II (21 CFR 872.3630, product code NHA). Manufacturing these components requires:
- ISO 13485:2016 certification — the quality management standard for medical device manufacturing
- Complete material traceability — mill certifications, certificates of conformance, and lot-level tracking throughout production
- FDA registration — required for manufacturers producing components that become part of a finished medical device
- ISO 14801 fatigue testing — FDA-recognized standard for dynamic fatigue testing of dental implants
For implant OEMs evaluating contract manufacturers, these aren't optional checkboxes — they're the baseline. Criterion holds ISO 13485:2016 certification and FDA registration, with full lot-level traceability managed through ProShop ERP from raw material receipt through final inspection.
Post-Machining Steps
Machined implant components don't go directly from the CNC machine to the patient. Post-machining steps include:
- Deburring — remove machining burrs that could affect fit or tissue contact
- Precision cleaning — remove cutting fluids, chips, and contamination
- Surface treatment — passivation or anodization to condition the TiO₂ layer
- Final inspection — CMM verification of dimensional conformance before release
Titanium vs. Zirconia: Choosing the Right Implant Material
Zirconia implants have gained traction as a metal-free alternative, particularly for patients with aesthetic concerns or reported metal sensitivities. Their white color eliminates the dark implant collar that can show through thinning gum tissue, and biocompatibility research is reasonably well-documented.
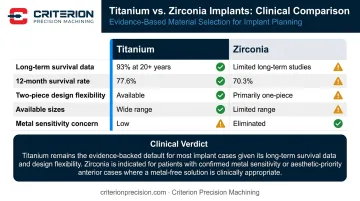
That said, the evidence base still favors titanium on most clinical dimensions:
| Factor | Titanium | Zirconia |
|---|---|---|
| Long-term survival data | 93% at 20+ years | Limited long-term studies |
| 12-month survival (2024 systematic review) | 77.6% | 70.3% |
| Two-piece design flexibility | Available — allows angular adjustment | Primarily one-piece, limiting placement flexibility |
| Available sizes and designs | Wide range | More limited |
| Metal sensitivity concern | Rare; hypersensitivity documented but uncommon | Not applicable |
The practical decision comes down to several clinical factors:
- Bone volume and density — titanium's wider size range accommodates more anatomical situations
- Patient allergy history — zirconia is a reasonable alternative where documented titanium sensitivity exists
- Aesthetic zone — zirconia's white color is an advantage in high-visibility anterior positions with thin gingival tissue
- Arch position — titanium's superior fatigue data makes it the conservative choice for high-load posterior sites
Titanium remains the default recommendation in most clinical scenarios. Zirconia is a valid, evidence-supported option for specific patient profiles — but clinicians should select it for documented clinical reasons, not as a general metal-free preference.
Frequently Asked Questions
What are titanium implants made of?
Most titanium dental implants use Grade 5 titanium alloy (Ti-6Al-4V ELI) — a blend of titanium, aluminum, and vanadium that delivers high tensile strength and excellent biocompatibility. Grade 4 commercially pure titanium is also used in certain implant designs where maximum biocompatibility is prioritized over peak mechanical strength.
Are titanium implants MRI safe?
Titanium is paramagnetic rather than ferromagnetic, so it doesn't interact meaningfully with MRI magnetic fields and doesn't produce significant imaging artifacts. Most titanium implants are MRI-compatible, though patients should confirm specific device labeling with their clinician before imaging.
What are the long-term effects of titanium implants?
Long-term outcomes are generally favorable: systematic review data shows 93% survival at 20+ years. The primary long-term considerations are peri-implantitis (affecting roughly 22% of patients) and rare titanium particle sensitivity — both manageable with routine monitoring and maintenance.
Can titanium implants be removed?
Yes, through implant explantation using reverse torque, trephine burs, or piezosurgery depending on osseointegration level and remaining bone. Because successful osseointegration makes removal more complex than placement, it's typically reserved for implant failure, infection, fracture, or malposition.
How long do titanium dental implants last?
Titanium implants can last 20 years or longer, and many patients retain them for life. Longevity depends on oral hygiene, bone density, systemic health conditions like diabetes, and whether peri-implantitis develops.
What is the difference between Grade 4 and Grade 5 titanium for dental implants?
Grade 4 is commercially pure titanium with moderate strength (550 MPa tensile) and maximum biocompatibility. Grade 5 (Ti-6Al-4V ELI) is an alloy with significantly higher tensile (860 MPa) and fatigue strength due to added aluminum and vanadium, making it the more common choice for load-bearing implant fixtures where mechanical demands are highest.