
Introduction
Cleanroom machining produces precision components in controlled environments that restrict airborne particles, microorganisms, and machining debris. These facilities hold strict limits on particulate count, temperature, and humidity — requirements that standard machine shops simply don't meet.
Not all medical device parts require cleanroom machining—but choosing incorrectly carries serious consequences. Manufacturing implantable components or patient-contact devices in uncontrolled environments can lead to FDA Form 483 observations, failed biocompatibility testing, product recalls, and most critically, compromised patient safety. Nearly 38% of medical device recalls stem from manufacturing issues, many linked to contamination that could have been prevented through appropriate environmental controls.
Knowing when your parts actually require a cleanroom — and when they don't — is one of the most consequential decisions in your manufacturing process.
Key Takeaways
- Cleanroom machining is required for Class II and Class III devices with patient contact, tight bioburden limits, or explicit regulatory requirements
- ISO 7 (Class 10,000) and ISO 8 (Class 100,000) are the most common cleanroom classifications for medical device machining
- Device classification, material biocompatibility, and contamination sensitivity trigger cleanroom requirements
- Non-compliance results in FDA warnings, failed biocompatibility tests, and product recalls
- Vet machining partners for ISO 13485 certification, FDA registration, and documented environmental monitoring
Why Cleanroom Machining Matters for Medical Device Components
Machining Processes Generate Contamination
CNC machining operations—cutting, milling, and turning—actively generate particulate contamination that differs from assembly-phase risks in kind, not just degree. Research on titanium alloy milling shows that machining generates both fine (0.5–2.5 µm) and coarse (2.5–10 µm) particles, with particle concentration and suspension time significantly influenced by cutting fluid type. Minimum Quantity Lubrication (MQL) systems, for example, generate high levels of airborne particles that remain suspended longer than flood cooling systems.
Metalworking fluids create additional contamination vectors. These fluids generate aerosols containing endotoxins—bacterial byproducts that trigger inflammatory responses. Studies show the majority of airborne endotoxin in metalworking fluid aerosols appears in the 2.5-10 µm size fraction, settling on device surfaces during machining operations.

Particles Embed in Component Surfaces
Uncontrolled particulates create bioburden risks by embedding in component surfaces, especially in complex geometries or porous materials. Research on titanium implants reveals that blasting particles like Al2O3 can remain embedded in surfaces even after cleaning, potentially causing adverse biological effects.
Three surface characteristics make embedding especially difficult to remediate:
- Internal channels, threads, and pockets trap machining debris and resist post-process cleaning
- Titanium, porous polymers, and textured surfaces retain both particles and cutting fluid residues
- Contamination in fine surface finishes disrupts the Ra values required for biocompatibility
Impact on Regulatory Approval
Surface contamination from non-cleanroom manufacturing is a primary cause of failure during FDA inspections and biocompatibility testing. Process contaminants—including cutting fluids, particles, and machine lubricants—must be evaluated as part of biological risk assessment under ISO 10993-1 standards.
Cleanroom environments control these risks by:
- Maintaining specific airborne particle limits per cubic meter
- Filtering air through HEPA systems (99.97% efficient at 0.3 µm)
- Controlling temperature and humidity to prevent condensation and microbial growth
- Implementing gowning protocols and material flow controls
- Monitoring environmental conditions continuously with documented validation
Cleanroom Machining vs. Cleanroom Assembly
Most articles address cleanroom assembly—packaging sterile devices in controlled environments. Cleanroom machining is a different problem entirely. Active material removal generates chips, dust, and aerosolized coolants continuously—each a direct challenge to air filtration systems that assembly operations simply don't create.
The distinction matters for qualification: environmental controls validated for assembly may not be sufficient for machining operations without additional engineering review.
When Medical Device Parts Require Cleanroom Machining
Cleanroom requirements hinge on three factors: device classification, patient contact level, and regulatory pathway. Not every medical part needs a controlled environment — but for those that do, the stakes are high.
Based on Device Classification and Patient Contact
FDA Device Classifications:
The FDA classifies medical devices into three categories based on risk:
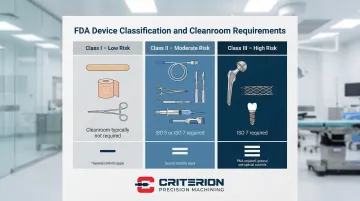
- Class I - Low risk, minimal regulatory controls (most don't require cleanroom manufacturing)
- Class II - Moderate risk, special controls required
- Class III - High risk, life-supporting or life-sustaining devices
FDA regulations under 21 CFR 820.70(c) mandate environmental controls where conditions could adversely affect product quality. Class II and Class III devices with patient contact typically require cleanroom manufacturing.
Direct vs. Indirect Contact:
Direct contact devices require stricter controls:
- Orthopedic implants (hip stems, spinal rods, bone plates)
- Catheter components contacting blood or internal tissues
- Surgical instrument tips entering sterile body cavities
- Drug delivery device parts contacting pharmaceuticals
Indirect contact devices may require cleanroom machining:
- Housings for sterile delivery systems
- External components of implantable devices
- Diagnostic equipment contacting bodily fluids
Examples Requiring Cleanroom Machining:
- Orthopedic implants and fixation devices
- Cardiovascular stents and catheter components
- Surgical tool tips and cutting edges
- Drug delivery device chambers and valves
- Dental implant components
Based on Material and Surface Requirements
Porous Materials:
Materials like porous titanium and PEEK require cleanroom machining to prevent particle entrapment. Research demonstrates that organic matter such as machine oil can contaminate titanium surfaces, with standard cleaning methods often failing to remove contamination from porous or textured surfaces.
Surface Finish Requirements:
Surface roughness (Ra values) directly impacts biocompatibility and contamination retention. Implantable devices typically require Ra values between 0.1-0.4 µm to prevent bacterial colonization, while rougher surfaces increase particle release risks.
Cleanroom environments prevent contamination that affects finish quality:
- Airborne particles settling on surfaces during finishing operations
- Coolant contamination from unfiltered shop air
- Cross-contamination from non-medical components machined in the same facility
Biocompatibility Testing (ISO 10993):
ISO 10993 standards explicitly require evaluation of process contaminants and residues, including cutting fluids, particles, and machine lubricants. Parts machined outside a cleanroom environment frequently fail biocompatibility testing — sending manufacturers back to square one with costly retesting and schedule delays.
Based on Regulatory and Sterilization Requirements
FDA 21 CFR Part 820 Requirements:
Federal regulations mandate documented environmental controls including:
- Procedures for controlling environmental conditions
- Periodic inspection of environmental control systems
- Documentation verifying systems are adequate and functioning properly
Terminal Sterilization Limitations:
Terminal sterilization — whether ethylene oxide (EtO), gamma radiation, or autoclave — cannot remove embedded particles introduced during machining. Three common methods, one shared limitation:
- EtO: Gas penetration is blocked by particle accumulation on surfaces
- Gamma radiation: Particulates can physically shield microorganisms from the dose
- Autoclave: Heat and steam can't dislodge particles trapped in surface features
Particulates that shield microorganisms from sterilizing agents can produce non-sterile products despite a validated sterilization cycle.
Bioburden Limits:
ISO 11737-1 defines bioburden as the sum of microbial contributions from raw materials, manufacturing processes, and the manufacturing environment. Cleanroom machining keeps bioburden within acceptable limits before sterilization, ensuring cycles achieve the required Sterility Assurance Level (SAL).
When bioburden runs high — or when resistant organisms are present — sterilization cycles must be intensified. That puts heat-sensitive materials and polymer-based components at risk of damage, a trade-off that cleanroom manufacturing helps avoid entirely.
ISO Classifications and What They Mean for Machined Components
ISO 14644-1 Classification Overview
ISO 14644-1:2015 defines cleanroom classifications based on airborne particle concentration per cubic meter. The standard measures particles at specific size thresholds, with stricter classes allowing fewer particles.
ISO Cleanroom Classification Table:
| ISO Class | Max Particles/m³ (≥0.5 µm) | Max Particles/m³ (≥1.0 µm) | Max Particles/m³ (≥5.0 µm) | Typical Medical Device Application |
|---|---|---|---|---|
| ISO 5 | 3,520 | 832 | 29 | Aseptic processing, critical implant assembly |
| ISO 6 | 35,200 | 8,320 | 293 | Sterile surgical instruments, invasive devices |
| ISO 7 | 352,000 | 83,200 | 2,930 | Medical device machining, implant manufacturing |
| ISO 8 | 3,520,000 | 832,000 | 29,300 | General controlled manufacturing, non-sterile devices |
Common Classifications for Medical Device Machining
ISO 7 (Class 10,000)
ISO 7 is the most common classification for medical device machining operations where components have direct patient contact or require stringent contamination control before terminal sterilization.
Practical requirements include:
- 60-90 air changes per hour (ACH) to maintain particle counts
- HEPA filtration rated 99.97% efficient at 0.3 µm particles
- Maximum 352,000 particles ≥0.5 µm per cubic meter at operational state
- Continuous particle counting with documented environmental monitoring records
ISO 8 (Class 100,000)
ISO 8 environments support general controlled manufacturing for components that will undergo rigorous downstream cleaning and sterilization, or for non-sterile devices where moderate environmental control is required.
Practical requirements include:
- 30-60 air changes per hour (ACH)
- HEPA filtration throughout the controlled zone
- Maximum 3,520,000 particles ≥0.5 µm per cubic meter at operational state
- Periodic particle monitoring with documented results
Cleanroom States: As-Built, At-Rest, and Operational
ISO 14644-1 defines three occupancy states that significantly impact classification:
- As-built: Installation complete with services functioning, but no equipment, materials, or personnel
- At-rest: Equipment installed and operating, but no personnel present
- Operational: Functioning in specified manner with personnel present and working
Why operational classification matters for machining: Machining operations generate significant particulates, challenging air filtration systems. A cleanroom may achieve ISO 7 at-rest but only ISO 8 operational during active machining. Verify your manufacturing partner's classification during actual production, not just static conditions.

Federal Standard 209E Equivalents
You may still encounter older Class designations in legacy specifications or supplier documentation. Although Federal Standard 209E was cancelled in 2001, it remains a common reference point:
- ISO 7 = Class 10,000 (10,000 particles ≥0.5 µm per cubic foot)
- ISO 8 = Class 100,000 (100,000 particles ≥0.5 µm per cubic foot)
Signs Your Medical Device Components Need Cleanroom Machining
Regulatory Feedback
FDA reviewers may request documentation of environmental controls during 510(k) or PMA submissions, particularly for:
- Class II devices with patient contact
- Class III implantable devices
- Devices with stringent bioburden requirements
- Components contacting sterile pharmaceuticals or biologics
Bioburden Testing Results
Contamination levels above acceptable limits for your sterilization process point to a manufacturing environment problem. If bioburden testing consistently shows elevated microbial counts or resistant organisms, cleanroom machining is likely what's needed to bring pre-sterilization bioburden within range.
Common red flags in bioburden results include:
- Counts trending upward across production lots
- Presence of resistant or spore-forming organisms
- Variability that exceeds your sterilization validation assumptions
Customer Specifications
Beyond internal test data, you may also face an external mandate. Quality agreements or customer specifications often explicitly require ISO-classified manufacturing environments — and medical device OEMs routinely build these requirements into supplier quality agreements. If your agreement calls out a specific cleanroom class, that requirement isn't negotiable at audit time.
What Happens When Cleanroom Standards Aren't Met
Regulatory Consequences
The FDA actively enforces environmental control requirements through inspections and warning letters.
Recent enforcement examples:
Phillips Precision, Inc. (2024) received a Warning Letter citing failure to validate cleaning processes and failure to maintain process control procedures. The FDA specifically noted metal debris, leftover burrs, and residue on machined devices, with corrective actions implemented without prior verification of effectiveness.
Form 483 observations commonly cite failure to leak-test HEPA filters, structural deficiencies in cleanroom construction, and inadequate cleaning of ISO 5 hoods.
Non-compliance can result in:
- FDA Form 483 observations during inspections
- Warning letters requiring corrective action
- Failure to achieve 510(k) clearance or PMA approval
- Consent decrees or facility shutdowns in severe cases
Product Quality Issues
Manufacturing in inadequate environments causes:
Triggers adverse biocompatibility responses — surface contamination from residual cutting fluids or particulates forces expensive retesting and delays. Approximately 5-10% of medical equipment undergoes safety recalls due to biocompatibility issues, with contamination frequently identified as the root cause.
Drives up bioburden, forcing more aggressive sterilization cycles that can damage heat-sensitive materials and polymer components.
Embeds particles that compromise surface finish, dimensional accuracy, and mechanical properties — turning a compliant part into a reject.
Commercial Impact
Those quality failures don't stay in the lab. The downstream business costs are just as serious:
- Recalls that damage customer relationships and generate significant remediation costs
- Parts rejected at incoming inspection, disrupting customer production schedules
- Lost contracts, as OEMs now routinely audit supplier facilities and require documented cleanroom capabilities
- Lasting reputation damage — the medical device supply chain is a small world, and quality problems travel fast

Selecting a Cleanroom Machining Partner
Baseline Certifications
Verify these foundational requirements:
- ISO 13485:2016: Non-negotiable for medical device work — ensures documented quality controls and processes specifically designed for medical device manufacturing, including cleanliness standards
- FDA Registration: Confirms compliance with 21 CFR Part 820 (FDA's Quality System Regulation); required for any manufacturer producing components for regulated devices
Quality Systems and Environmental Controls
Evaluate documented quality systems including:
- Environmental monitoring protocols: Documented particle counting schedules, temperature/humidity monitoring, and microbial sampling
- Validation protocols: Evidence of cleanroom qualification (IQ/OQ/PQ) and periodic revalidation
- Cleaning procedures: Validated cleaning processes for equipment, tools, and components
- Personnel training: Gowning procedures, contamination control practices, and cleanroom behavior protocols
Request documentation showing:
- Particle count data from operational states (not just at-rest)
- Environmental monitoring trending over time
- Corrective actions taken when excursions occur
- Calibration records for particle counters and monitoring equipment
Machining Capabilities
Assess technical capabilities specific to your needs:
Precision tolerances: Medical device components typically require ±0.0002" or tighter — confirm the shop holds this routinely, not just on showcase parts.
Material expertise: Confirm hands-on experience with:
- Titanium (Ti6Al4V, commercially pure grades)
- Surgical-grade stainless steels (316L, 17-4 PH)
- PEEK and high-performance polymers
- Nitinol for cardiovascular applications
Complex geometry experience: Confirm capability with:
- Internal channels and cross-holes
- Fine threads and precision features
- Micro-components (sub-millimeter dimensions)
- Multi-axis machining for complex contours
Proven Track Record
Consider partners with:
- Experience serving zero-defect industries — medical device, aerospace, and defense — where long production histories indicate sustained quality, not just passing audits
- Inspection infrastructure that matches your requirements: CMM with PC-DMIS, optical systems, and documented measurement uncertainty
- Established OEM relationships that you can verify — customer names and references carry more weight than self-reported claims
Criterion Precision Machining, operating since 1953, holds ISO 13485 and FDA registration and has supplied components to OEMs including Smith & Nephew and Riverpoint Medical. That kind of track record is worth asking any prospective partner to match.
Frequently Asked Questions
What are the cleanroom requirements for medical devices?
Class II and Class III devices with patient contact typically require ISO 7 or ISO 8 environments under FDA 21 CFR Part 820. Specific requirements depend on device risk profile, sterilization method, and bioburden limits — and must be supported by documented environmental monitoring and validated cleaning procedures.
What are the requirements for ISO 7 cleanroom?
ISO 7 cleanrooms must maintain a maximum of 352,000 particles ≥0.5 microns per cubic meter during production. This requires HEPA filtration, 60-90 air changes per hour, controlled temperature and humidity, and verified particle counts under operational (not just static) conditions.
What is ISO 7 equivalent to?
ISO 7 is equivalent to Federal Standard 209E Class 10,000, meaning 10,000 particles of 0.5 microns or larger per cubic foot. Although Federal Standard 209E was officially cancelled in 2001, the Class 10,000 designation remains a common industry reference for cleanroom classification.
What is the ISO standard for CNC?
There's no specific "ISO standard for CNC" machining. However, CNC machining for medical devices must occur in environments meeting ISO 14644-1 classifications (typically ISO 7 or ISO 8) when required by device specifications, regulatory requirements, or customer quality agreements. The ISO 14644-1 standard defines cleanroom classifications based on airborne particulate limits.
What is cleanroom manufacturing?
Cleanroom manufacturing is production in controlled environments with defined limits on airborne particles, temperature, humidity, and microbial contamination. For medical devices, it encompasses environmental monitoring, validated cleaning procedures, personnel gowning protocols, and documented quality systems — all working together to ensure consistent contamination control.
When is cleanroom machining required for medical device components?
Cleanroom machining is required when device classification, bioburden limits, or customer specifications demand controlled environments. The clearest triggers are direct patient contact, implantable components, porous materials prone to particle entrapment, and parts that interface with sterile pharmaceuticals or biologics.


